





晴れましたね。クリスマス近いいでたち。これから講演に向かいます。

It’s cleared up nicely. I’m dressed for the Christmas season now. I’m on my way to a lecture.

 藤本幸弘オフィシャルブログ
藤本幸弘オフィシャルブログ
晴れましたね。クリスマス近いいでたち。これから講演に向かいます。
It’s cleared up nicely. I’m dressed for the Christmas season now. I’m on my way to a lecture.
美容機器の「安定性」とは何か
――派手さの裏側で、臨床を支えているもの――
学会会場を歩いていると、いつも同じ光景に出会う。
ブースの中央には、最新機種。
大型スクリーンには、劇的なビフォーアフター。
そして耳に心地よい言葉が並ぶ。
「最短」「最強」「最新」「ノーダウンタイム」。
だが、長年この世界を歩いてきた者ほど、自然と足が止まるのは別の場所だ。
「その機械は、何年同じ出力を出し続けられるのか」
ここに、美容機器の本質がある。
安定性とは「効く」ことではない
美容医療における機器の安定性は、しばしば誤解される。
それは「強い出力が出る」ことでも、「一回で変化が出る」ことでもない。
安定性とは、同じ条件で、同じ結果が、長期間再現できること。
レーザー、RF、HIFEM、超音波。
どのエネルギーデバイスであっても、生体に与える刺激は「量」と「時間」で決まる。この二つが毎回微妙にズレれば、臨床結果もズレる。
実際、レーザー医療の基礎論文では、“energy stability over time” が治療成績に直結することが繰り返し示されている。
たとえば Anderson & Parrish による選択的光熱融解理論の後続研究では、設定値と実測値の乖離が、組織反応のばらつきを生むことが指摘されている
(Lasers in Surgery and Medicine, 1983; 1: 263–276)。
出力の安定性は「内部構造」で決まる
国際学会を巡ると、同じ波長・同じスペックを謳う機器が溢れている。
しかし分解写真を見ると、内部構造はまったく異なる。
電源部の余裕設計
冷却系の冗長性
センサーのフィードバック精度
キャリブレーション頻度
これらはカタログにはほとんど書かれない。
だが、5年後、10年後の安定性を決めるのはここだ。
RFデバイスに関するレビューでは、
出力制御のフィードバック機構がない機器ほど、
長期使用でエネルギー誤差が拡大することが報告されている
(Gold et al., Dermatologic Surgery, 2011; 37: 889–898)。
生体側から見た「安定性」
もう一つ重要なのは、生体の側だ。
人間の皮膚は、日によって状態が違う。
年齢、ホルモン、睡眠、炎症。
それでも結果を揃えるためには、機械側がブレないことが絶対条件になる。
ここでも鍵になるのは「最大出力」ではなく、毎回同じ刺激を届けられるかという一点だ。
安定性は「地味」だが、裏切らない
派手な新製品は、確かに楽しい。展示会場では人だかりもできる。だが、10年後も診療室の片隅で静かに稼働しているのは、
たいてい“地味な顔”の機械だ。
長期フォローアップ研究では、初期効果よりも合併症率と再現性が最終的な評価を決めることが示されている
(Alster & Tanzi, Lasers in Surgery and Medicine, 2004; 34: 241–247)。
美容医療は、短距離走ではない。患者さんの人生に伴走する、長い時間の医療だ。
リバースエンジニアリングと後発品
——「似せる技術」と「積み上げる技術」の決定的な違い——
学会の展示会場を歩いていると、
ある瞬間に、ふと足が止まることがある。
「……あれ? これ、見たことがある構造だな」
筐体の曲線、ハンドピースの重量感、
UIの配置、説明の言い回しまで、どこか既視感がある。
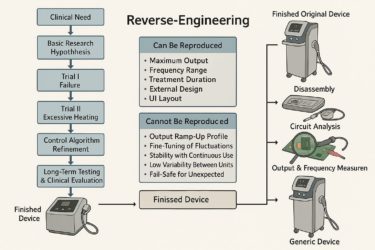
それが、リバースエンジニアリングによって生まれた後発品だ。
リバースエンジニアリングとは何か
リバースエンジニアリングとは、
完成した製品を分解・解析し、
形状
材質
出力
回路構成
を後追いで再構築する技術を指す。
工学的には、決して違法でも邪道でもない。
航空機、半導体、自動車産業でも日常的に行われている。
問題は、医療機器、とくにエネルギーデバイスにこれを適用したときに起きる。
医療機器で「再現できないもの」
後発品メーカーが再現できるのは、主に以下だ。
最大出力値
周波数レンジ
照射時間
外形寸法
いわば「静止した数値」である。
しかし、臨床で効いているのは、
数値ではなく挙動だ。
出力の立ち上がり速度
微細な揺らぎ(フラクチュエーション)
連続使用時のドリフト
温度・負荷変化に対する補正
安全域に入る直前の制御ロジック
これらは、
分解しても分からない
マニュアルにも書いていない
長年の失敗と改良の履歴そのもの
つまり、時間の層だ。
リバースエンジニアリングは、
「形」は真似できても、
「時間」は真似できない。
後発品が抱える構造的限界
後発品が臨床で問題を起こしやすい理由は、
技術力不足というより、開発プロセスの省略にある。
本来、オリジナル機器は
基礎実験
動物試験
ヒト初期試験
不具合の修正
再設計
長期使用テスト
という、遠回りの塊でできている。
後発品は、この②〜⑤を
「市場で埋め合わせる」構造になる。
結果として、
個体差が大きい
ロットごとに挙動が違う
長時間使用で不安定化
トラブル対応が後手に回る
という現象が起きる。
FDAも医療機器後発化について、
医療機器における同等性評価は、
工学的同等性を示すものであり、
臨床的同一性を保証するものではない
U.S. FDA, Guidance for Industry, 2018
と明確に述べている。
旅を続けてわかったこと
ヨーロッパでも、アメリカでも、アジアでも。
評価され続けているメーカーに共通するのは、
「安定性を哲学として持っているかどうか」だった。
新しいことをしない、という意味ではない。むしろ逆だ。変わり続けるために、変えてはいけない核を守っている。
—What Truly Supports Clinical Practice Behind the Flash—
When walking through the halls of a medical conference, one is always greeted by the same scene.
At the center of each booth stands the latest model.
Large screens display dramatic before-and-after images.
And a series of pleasant-sounding words fills the air:
“Fastest,” “Most powerful,” “Latest,” “No downtime.”
Yet the longer one has walked this path, the more naturally one’s feet stop elsewhere.
At a different question entirely:
“How many years can this machine continue to deliver the same output?”
Here lies the essence of aesthetic medical devices.
Stability in aesthetic medicine is often misunderstood.
It does not mean “high output,” nor does it mean “visible change in a single session.”
Stability means that, under the same conditions, the same results can be reproduced consistently over a long period of time.
Laser, RF, HIFEM, ultrasound—
Regardless of the energy modality, the biological stimulus is determined by dose and time.
If either fluctuates even slightly from session to session, clinical outcomes will inevitably fluctuate as well.
Indeed, foundational laser medicine literature has repeatedly shown that energy stability over time directly correlates with treatment outcomes.
For example, follow-up studies to the theory of selective photothermolysis proposed by Anderson and Parrish point out that discrepancies between set values and actual measured output lead to variability in tissue response
(Lasers in Surgery and Medicine, 1983; 1: 263–276).
At international congresses, devices claiming the same wavelength and specifications are everywhere.
Yet when one examines teardown images, their internal structures differ completely.
Power supply headroom
Redundancy in cooling systems
Precision of sensor feedback
Calibration frequency
These factors are rarely mentioned in brochures.
However, they are precisely what determine stability five or ten years later.
A review of RF devices reports that systems lacking output-feedback control mechanisms exhibit increasing energy deviation with long-term use
(Gold et al., Dermatologic Surgery, 2011; 37: 889–898).
Another crucial aspect is the patient’s body.
Human skin changes from day to day.
Age, hormones, sleep, inflammation—all fluctuate.
To achieve consistent outcomes despite this, the machine itself must remain unwavering.
Once again, the key is not maximum output, but whether the device can deliver the same stimulus every single time.
Flashy new products are undeniably exciting. Crowds gather around them at exhibitions.
But ten years later, the machines still quietly operating in the corner of the clinic are usually the ones with the most unassuming appearance.
Long-term follow-up studies demonstrate that complication rates and reproducibility, rather than initial effects, ultimately determine clinical evaluation
(Alster & Tanzi, Lasers in Surgery and Medicine, 2004; 34: 241–247).
Aesthetic medicine is not a sprint.
It is a long-distance practice—one that walks alongside a patient’s life.
—The Decisive Difference Between “Imitation” and “Accumulation”—
While walking through conference exhibition halls, there are moments when one suddenly stops.
“…Wait—haven’t I seen this structure before?”
The curvature of the housing, the weight of the handpiece,
the UI layout, even the phrasing of the explanations—
all feel strangely familiar.
This is the hallmark of products born through reverse engineering.
Reverse engineering refers to the process of disassembling and analyzing a completed product in order to reconstruct:
Shape
Materials
Output
Circuit configuration
From an engineering standpoint, it is neither illegal nor unethical.
It is routinely practiced in aviation, semiconductors, and the automotive industry.
The problem arises when this approach is applied to medical devices—particularly energy-based devices.
What follow-on manufacturers can reproduce are mainly the following:
Maximum output values
Frequency ranges
Irradiation time
External dimensions
In other words, static numbers.
But what truly works in clinical practice is not numbers—it is behavior.
Output ramp-up speed
Micro-fluctuations
Drift during continuous use
Compensation for temperature and load changes
Control logic just before entering safety thresholds
These elements:
Cannot be understood through disassembly
Are not written in manuals
Represent the accumulated history of failures and refinements
They are, in essence, layers of time.
Reverse engineering can imitate form,
but it cannot imitate time.
The reason follow-on devices are more prone to clinical issues lies not so much in technical inferiority as in the omission of the development process.
Original devices are built through a long detour of:
Basic experiments
Animal studies
Early human trials
Failure correction
Redesign
Long-term durability testing
Follow-on products effectively outsource steps ②–⑤ to the market itself.
As a result:
Individual variability increases
Behavior differs between production lots
Stability deteriorates with prolonged use
Troubleshooting becomes reactive rather than proactive
The FDA has also clearly stated regarding medical device equivalence:
“Substantial equivalence determinations demonstrate engineering equivalence,
not clinical sameness.”
(U.S. FDA, Guidance for Industry, 2018)
In Europe, America, and Asia alike, manufacturers that continue to be respected share one common trait:
They hold stability as a philosophy.
This does not mean they avoid innovation—quite the opposite.
They protect the unchanging core precisely so that they can continue to evolve.
日銀利上げを読み解く、三つの要素——
日銀が19日の利上げの発表を考えていると報道がありました。
「日銀は18〜19日に開く金融政策決定会合で政策金利を現在の0.5%から引き上げる最終調整に入る。0.25%引き上げて0.75%とする案が有力で、1995年以来30年ぶりの金利水準に達することになる。
植田和男総裁ら執行部は利上げの議案を提出する意向を示唆している。日本経済新聞社の取材では、正副総裁を含めて9人の政策委員のうち過半数が執行部案を支持する見通しだ。」
日銀が利上げした場合
基本シナリオは「円高・株安」
ただし、短期と中長期、業種別で動きは分かれる、ここが重要です。
①為替:なぜ円高になるのか
日銀が利上げすると、
日本の金利 ↑
日米金利差 ↓
円を売ってドルを買う理由が弱まる
その結果、
円安トレンドは止まり、円高方向に振れやすくなります。
実際、金利と為替の関係は非常に教科書的です。
これまで円は、「持っているだけで損をする通貨」だった。
だから売られ続けた。
利上げは、その前提を静かに崩す。
円安は加速するのではない。
止まり、揺り戻される余地が生まれる。
② 株式市場:なぜ株安になりやすいのか
● 短期(最初の反応)
金利上昇 → 企業の借入コスト ↑
割引率 ↑ → 株価の理論価値 ↓
そのため全体指数(日経平均・TOPIX)は下がりやすい。
利上げのニュースが出ると、
株式市場はまず売る。
これは恐怖というより、
再計算だ。
株安とは、
崩壊ではない。
見直しである。
要素③ 時間 —— 短期と長期は、別の物語
多くの誤解は、
「今」と「これから」を混ぜてしまうことから生まれる。
短期では、
円は乱高下し
株は不安定になる
だが時間を置くと、景色は変わる。
金利が“ある世界”では、
企業の体力差が見える
為替に頼らない経営が評価される
市場の質が上がる
利上げとは、
未来を壊す行為ではない。
時間を取り戻す政策だ。
▲ 下がりやすい
輸出企業(自動車・電機)
→ 円高=利益圧迫
高PERグロース株
→ 金利上昇に弱い
▲ 上がりやすい/耐性がある
銀行・保険
→ 金利マージン改善
内需・ディフェンシブ
→ 為替影響が小さい
金利。
株価。
そして時間。
それらを混ぜないこと。
そこから、
本当の理解が始まる。
Reports have emerged that the Bank of Japan (BOJ) is considering announcing an interest rate hike on the 19th.
“The Bank of Japan is entering the final stage of coordination to raise the policy interest rate from the current 0.5% at its Monetary Policy Meeting scheduled for the 18th–19th. A 0.25 percentage point increase to 0.75% is seen as the most likely option, which would bring interest rates to a level not seen in 30 years, since 1995.
Governor Kazuo Ueda and other members of the executive leadership have signaled their intention to submit a proposal for a rate hike. According to reporting by Nikkei, a majority of the nine policy board members, including the deputy governors, are expected to support the executive proposal.”
The baseline scenario is:
a stronger yen and weaker equities.
However, this is where nuance matters.
Market reactions differ between the short term and the medium-to-long term, and by sector.
When the BOJ raises interest rates:
Japanese interest rates ↑
The Japan–U.S. interest rate differential ↓
The incentive to sell yen and buy dollars weakens
As a result, the yen’s depreciation trend is likely to stall and tilt toward appreciation.
In fact, the relationship between interest rates and exchange rates is highly textbook.
Until now, the yen had been a currency that “cost money simply to hold.”
That is why it continued to be sold.
A rate hike quietly dismantles that assumption.
The yen’s weakness does not accelerate.
Instead, it pauses—and creates room for a corrective rebound.
Interest rates rise → corporate borrowing costs increase
Discount rates rise → the theoretical value of equities declines
As a result, broad indices such as the Nikkei 225 and TOPIX tend to fall.
When news of a rate hike emerges,
the stock market sells first.
This is not fear—
it is recalculation.
A market decline does not mean collapse.
It means reassessment.
Many misunderstandings arise from conflating
“now” with “what comes next.”
In the short term:
the yen fluctuates sharply
equities become unstable
But with time, the landscape changes.
In a world where interest rates exist:
differences in corporate financial strength become visible
management that does not rely on currency depreciation is rewarded
overall market quality improves
A rate hike is not an act that destroys the future.
It is a policy that restores time.
Exporters (automobiles, electronics)
→ A stronger yen compresses profits
High-PER growth stocks
→ Vulnerable to rising interest rates
Banks and insurance companies
→ Improved interest margins
Domestic demand & defensive sectors
→ Limited exposure to exchange-rate movements
Interest rates.
Stock prices.
And time.
Do not mix them together.
From that separation,
true understanding begins.
ビタミンCという“扱いにくい優等生”の全体像ー
ビタミンCという、もっとも誤解されている分子について
国際学会の展示会場を歩いていると、必ずどこかで目に入る単語がある。
Vitamin C。
あまりにも身近で、あまりにも安価で、あまりにも「分かったつもり」になりやすい栄養素だ。
だが、この分子ほど評価が二極化している存在も珍しい。
「風邪に効く」「美白にいい」「がんを治す」「いや、何も効かない」——どれも半分は正しく、半分は間違っている。
1. ビタミンCは「抗酸化物質」では終わらない
教科書的には、ビタミンC(アスコルビン酸)は水溶性抗酸化物質として説明される。
しかし近年の研究では、その本質は酸化還元制御を通じた細胞環境の調律因子であることが明らかになってきた。
たとえば、コラーゲン合成。
これは美容の話ではなく、血管壁・骨・皮膚・腱すべてに関わる基礎生理だ。
ビタミンCはプロリン・リジン水酸化反応の補酵素
欠乏すると壊血病=「結合組織の崩壊」が起きる
この古典的事実は、今なお変わらない。
Peterkofsky B. “Ascorbate requirement for hydroxylation and secretion of procollagen”
The Journal of Biological Chemistry, 1972; 247: 153–159.
2. 「風邪に効く」は、正確にはこういう意味だ
ビタミンCが風邪を治すというエビデンスは弱い。
しかし、「重症化と罹病期間を短縮する」という点では、かなり一貫したデータが存在する。
特に、
強い身体的ストレス
寒冷環境
長距離移動・睡眠不足
こうした条件下では、免疫細胞内のビタミンC消費量が急増する。
メタアナリシスの結論は冷静だ。
Hemilä H, Chalker E.“Vitamin C for preventing and treating the common cold”Cochrane Database of Systematic Reviews, 2013; Issue 1: CD000980, pp. 1–135.
「万能ではないが、ゼロでもない」。科学が最も好む結論である。
3. 高濃度ビタミンC点滴は、なぜ議論になるのか
静脈内高濃度ビタミンC(IVC)は、経口摂取では到達できない血中濃度を実現する。
ここで初めて、ビタミンCは
抗酸化物質から
条件付きのプロオキシダント(過酸化水素産生)
へと性質を変える。
このメカニズムは、がん細胞の脆弱性を突く可能性があるとして研究が続いている。
Chen Q et al.“Pharmacologic ascorbic acid concentrations selectively kill cancer cells”Proceedings of the National Academy of Sciences USA, 2005; 102: 13604–13609.
ただし、
これは「治療」ではなく「補助的戦略」の域を出ていない。
魔法の弾丸ではないが、無視できる分子でもない。
4.ビタミンCは“効くか効かないか”で語るものではない
ビタミンCは、欠乏すれば確実に壊れる
過剰に期待すると裏切られる
その中間に、正しく使えば確実に仕事をする領域がある。
サプリメント売り場の派手なコピーでも、
SNSの極端な成功談でもなく、
「どの濃度で、どの時間軸で、どの生理現象に関わるのか」。
それを考えるのが、医療であり、科学だ。
★前提:ビタミンCは「抗酸化サプリ」ではない
最初にここを外すと、すべてがずれます。
ビタミンCは
単なるROS消去剤
ではなく
生体反応を成立させるための調節因子(redox regulator)
抗酸化作用は「結果」であって「本質」ではありません。
Levine M et al.
JAMA, 1999; 281(15): 1415–1423.
★加齢(35歳以降)とSOD低下という現実35歳前後から、ミトコンドリア由来スーパーオキシド増加
Cu/Zn-SOD、Mn-SOD活性低下
ROS処理の初段階が詰まり始める
これは老化研究ではほぼコンセンサスです。
Rikans LE, Hornbrook KR.
Biochim Biophys Acta, 1997; 1362: 116–127.
ここで重要なのは、
SODが落ちた=抗酸化を強化すればよい、ではない
SODは単なる消去酵素ではなく、
シグナル生成装置でもあるからです。
★スーパーオキシドは「悪」ではない
スーパーオキシドは
免疫初動反応
ミトコンドリア新生
運動適応
細胞ストレス応答
のトリガー。
過剰は害だが、過少は「生体が鈍る」。
Ristow M et al.
PNAS, 2009; 106(21): 8665–8670.
だから抗酸化は
アクセルではなくショックアブソーバー。
★ビタミンCの本当の仕事
臨床的に重要なのは、抗酸化よりこちら。
コラーゲン合成(皮膚・血管・腱)
カルニチン合成(疲労耐性)
カテコールアミン合成(ストレス応答)
HIF-1α制御(低酸素適応)
つまり
「肌がいい」「回復が早い」「疲れにくい」は、
ROS消去ではなく酵素反応が回っている結果。
Pullar JM et al.
Nutrients, 2017; 9(8): 866.
★ビタミンC(アスコルビン酸)の免疫調節作用
Vitamin C (Ascorbic acid, C₆H₈O₆)
ビタミンCは免疫細胞内に高濃度で取り込まれ、
抗ウイルス応答の維持および炎症反応の調整に関与する。
樹状細胞(Dendritic cell)
抗ウイルス因子の産生を支持
炎症性サイトカイン(IL-1β、IL-6)の過剰産生を抑制
→ 自然免疫と獲得免疫の橋渡し機能の安定化
マクロファージ(Macrophage)
抗ウイルス応答能の維持
活性化に伴う過剰炎症(IL-1β、IL-6)の制御
→ 感染防御と炎症収束のバランス調整
T細胞(T cell)
細胞増殖の支持
細胞障害活性(cytotoxicity)の維持
IFN-γ、IL-2、IL-17 などのサイトカイン産生を適正化
→ 過不足のない細胞性免疫応答
B細胞(B cell)
細胞増殖の支持
抗体産生能の維持
→ 液性免疫の質的安定化
全体としての位置づけ
免疫反応が破綻しないように整える
★用量の整理
生理学的に意味のあるラインは明確です。
用量 意味
~100 mg 欠乏回避
100–200 mg 生理最適・白血球飽和
300–1000 mg 短期・戦術的高用量
≥1000 mg 常用 大量摂取域
Levine M et al.
PNAS, 1996; 93(8): 3704–3709.
200 mgを超えると
吸収率低下
尿中排泄増加
効果は頭打ち
「たくさん飲んでいる安心感」の多くは、
腎臓を通過して消えている。
分割して飲むべき。
★大量摂取の問題点
1 g超を常用すると、
生理的ROSシグナル抑制
運動適応低下
免疫初動鈍化
下痢・腹部症状
鉄吸収過剰(フェリチン高値では逆効果)
IOMはULを2,000 mg/日に設定。
Institute of Medicine, 2000; pp.95–185.
★プロオキシダントに転ぶ条件
遊離ビタミンCという“扱いにくい優等生”の全体像
遊離鉄・銅があると、ビタミンCはFenton反応を促進。
フェリチン高値
鉄剤併用
ヘモクロマトーシス
では大量摂取は理論的に危険。
Halliwell B, Gutteridge JMC.
Arch Biochem Biophys, 1990; 280: 1–8.
★抗酸化は「ネットワーク」
ビタミンC単独では完結しない。
ビタミンE再還元
グルタチオン
NADPH
これらが揃って初めて意味を持つ。
Cだけ多い状態は、
非対称な抗酸化状態を生む。
Packer L et al.
Free Radic Biol Med, 1997; 22(4): 663–677.
★静注ビタミンCは別次元
経口と静注は薬理学的に別物。
静注では
血中ミリモル濃度
がん細胞選択的プロオキシダント
これは
日常サプリ議論とは完全に切り離す話。
Chen Q et al.
PNAS, 2005; 102(38): 13604–13609.
★最終まとめ
ビタミンCは抗酸化薬ではない
35歳以降、欠乏させない意義はある
一度に200 mg前後が基準線
高用量は「短期・戦術的」に
グラム単位常用は中庸を外れる
そして何より、
効くものほど、使いすぎない設計が必要
レーザー治療とまったく同じです。
万能に見えるものほど、プロの采配が問われる。
ビタミンCは「飲むか飲まないか」ではなく、どう位置づけるかで評価が決まる介入だと思います。

When walking through the exhibition halls of international scientific conferences, there is a word you will inevitably encounter somewhere:
Vitamin C.
It is so familiar, so inexpensive, and so easy to assume we already “understand” it.
Yet few molecules provoke such polarized evaluations.
“Effective against colds,” “good for skin whitening,” “cures cancer,” “no effect at all” — each of these claims is half true and half wrong.
Textbooks typically describe vitamin C (ascorbic acid) as a water-soluble antioxidant.
However, recent research has clarified that its essential role lies in regulating the cellular environment through redox control.
Take collagen synthesis, for example.
This is not merely a cosmetic concern; it is fundamental physiology involving blood vessel walls, bones, skin, and tendons.
Vitamin C acts as a cofactor in proline and lysine hydroxylation
Deficiency leads to scurvy — the collapse of connective tissue
This classical fact remains unchanged.
Peterkofsky B.
“Ascorbate requirement for hydroxylation and secretion of procollagen”
The Journal of Biological Chemistry, 1972; 247: 153–159.
Evidence that vitamin C cures the common cold is weak.
However, consistent data show that it reduces disease severity and shortens duration.
This effect is particularly evident under conditions such as:
Intense physical stress
Cold exposure
Long-distance travel or sleep deprivation
Under these conditions, vitamin C consumption within immune cells rises sharply.
The conclusion of a major meta-analysis is appropriately restrained:
Hemilä H, Chalker E.
“Vitamin C for preventing and treating the common cold”
Cochrane Database of Systematic Reviews, 2013; Issue 1: CD000980.
“Not a panacea, but not zero.”
This is the conclusion science favors most.
High-dose intravenous vitamin C (IVC) achieves blood concentrations unattainable by oral intake.
At this point, vitamin C shifts from:
an antioxidant
to
a conditional pro-oxidant (via hydrogen peroxide generation).
This mechanism is being studied for its potential to exploit vulnerabilities in cancer cells.
Chen Q et al.
“Pharmacologic ascorbic acid concentrations selectively kill cancer cells”
PNAS, 2005; 102: 13604–13609.
That said, this approach remains adjunctive, not curative.
It is not a magic bullet — but neither is it a molecule to dismiss.
Vitamin C:
If deficient, the body undeniably deteriorates
If overestimated, it disappoints
Between these extremes lies a zone where it performs reliably when used correctly.
Not flashy supplement marketing.
Not extreme success stories on social media.
But rather:
At what concentration, over what time scale, and in which physiological processes does it act?
That is the realm of medicine and science.
Miss this point, and everything becomes misaligned.
Vitamin C is not merely a ROS scavenger,
but a redox regulator that enables biological reactions.
Its antioxidant effect is a consequence, not its essence.
Levine M et al.
JAMA, 1999; 281(15): 1415–1423.
From around age 35:
Mitochondrial superoxide production increases
Cu/Zn-SOD and Mn-SOD activities decline
The first stage of ROS processing becomes congested
This is near-consensus in aging research.
Rikans LE, Hornbrook KR.
Biochim Biophys Acta, 1997; 1362: 116–127.
Importantly:
Reduced SOD does not mean antioxidants should simply be increased.
SOD is not merely a disposal enzyme — it is also a signal generator.
Superoxide triggers:
Innate immune activation
Mitochondrial biogenesis
Exercise adaptation
Cellular stress responses
Excess is harmful.
Deficiency makes the organism sluggish.
Ristow M et al.
PNAS, 2009; 106(21): 8665–8670.
Thus, antioxidants are not an accelerator —
they are shock absorbers.
Clinically, these roles matter more than antioxidation:
Collagen synthesis (skin, vessels, tendons)
Carnitine synthesis (fatigue resistance)
Catecholamine synthesis (stress response)
HIF-1α regulation (hypoxia adaptation)
“Better skin,” “faster recovery,” and “less fatigue”
are results of functional enzymatic reactions, not ROS elimination.
Pullar JM et al.
Nutrients, 2017; 9(8): 866.
Vitamin C (Ascorbic acid, C₆H₈O₆) accumulates at high concentrations in immune cells, contributing to antiviral defense and inflammatory regulation.
Dendritic cells
Support antiviral factor production
Suppress excessive IL-1β and IL-6
→ Stabilize the bridge between innate and adaptive immunity
Macrophages
Maintain antiviral competence
Control excessive inflammatory activation
→ Balance defense and resolution
T cells
Support proliferation
Maintain cytotoxicity
Optimize IFN-γ, IL-2, IL-17 production
→ Balanced cellular immunity
B cells
Support proliferation
Maintain antibody production
→ Stability of humoral immunity
Overall role:
Maintaining immune responses without breakdown.
Physiologically meaningful ranges are clear:
| Dose | Meaning |
|---|---|
| ≤100 mg | Deficiency prevention |
| 100–200 mg | Physiological optimum / leukocyte saturation |
| 300–1000 mg | Short-term, tactical high dose |
| ≥1000 mg | Chronic high-intake range |
Levine M et al.
PNAS, 1996; 93(8): 3704–3709.
Above 200 mg:
Absorption declines
Urinary excretion increases
Effects plateau
Much of the “reassurance” of high intake simply passes through the kidneys.
Divided dosing is preferable.
Regular intake above 1 g may lead to:
Suppression of physiological ROS signaling
Reduced exercise adaptation
Blunted immune initiation
Diarrhea and GI symptoms
Excess iron absorption (counterproductive with high ferritin)
The IOM sets the UL at 2,000 mg/day.
Institute of Medicine, 2000; pp. 95–185.
In the presence of free iron or copper, vitamin C promotes Fenton reactions.
High ferritin
Iron supplementation
Hemochromatosis
In such cases, large doses are theoretically risky.
Halliwell B, Gutteridge JMC.
Arch Biochem Biophys, 1990; 280: 1–8.
Vitamin C does not work alone.
Vitamin E recycling
Glutathione
NADPH
Only together do they function properly.
Excess vitamin C alone creates an imbalanced antioxidant state.
Packer L et al.
Free Radic Biol Med, 1997; 22(4): 663–677.
Oral and IV vitamin C are pharmacologically distinct.
IV administration achieves:
Millimolar plasma concentrations
Selective pro-oxidant effects in cancer cells
This discussion is entirely separate from everyday supplement use.
Chen Q et al.
PNAS, 2005; 102(38): 13604–13609.
Vitamin C is not an antioxidant drug
Preventing deficiency after age 35 has value
~200 mg per dose is a reasonable baseline
High doses should be short-term and tactical
Chronic gram-level intake lacks balance
And above all:
The more effective something is, the more carefully it must be designed.
This is exactly the same principle as laser therapy.
The more powerful it appears, the more professional judgment it requires.
Vitamin C is not about “taking it or not,”
but about how it is positioned as an intervention.
科学はSNSに負けたように見える
——それでも、エビデンスを手放してはいけない理由——
SNSを眺めていると、
科学はいつも負けているように見える。
「危険です!」
「これで治る!」
「医者は教えてくれない最新療法!」
どれも短く、強く、感情を揺さぶる。
一方で、科学の言葉は遅く、長く、慎重だ。
だから錯覚する。
——科学は時代遅れになったのではないか、と。
だが、それは事実ではない。
★科学は「勝つため」に作られていない
まず大前提として、
科学はSNSで勝つために存在していない。
科学が大切にしているのは、
• 再現できるか
• 他でも同じ結果が出るか
• 偶然ではないか
• 条件が変わっても成り立つか
つまり、個人の感動より、社会全体の安全だ。
この姿勢は、
どうしても言葉を鈍くする。
「必ず効く」と言えない。
「副作用はない」と言えない。
「全員に同じ結果」とも言えない。
それは弱さではなく、
責任を引き受けている証拠だ。
★治療法で煽るのも、恐怖で煽るのも、同じ構造です。
違うのは符号だけ。
片方は「希望」、もう片方は「不安」。
どちらも、人間の脳が最も強く反応するスイッチを押している。
★ナイスショットは「売りやすい」
ゴルフで言えば、
• 100打のうち99打は平凡
• 1打だけ、完璧なショットが出る
SNSが切り取るのは、
必ずその1打だ。
• この治療で治った
• この方法で人生が変わった
• これを知らないと危険
全体像も、
スコアカードも、
再現性も、
すべて省略される。
残るのは、
気持ちよく信じられる一瞬だけ。
★恐怖も、希望も「思考を省略させる」
恐怖は言う。
「考えるな、避けろ」
希望は言う。
「考えるな、信じろ」
方向は逆だが、
脳に起きていることは同じだ。
• 比較しない
• 条件を見ない
• 確率を考えない
だから、
恐怖で煽る話も、
新しい治療法も、
SNSでは同じ速度で広がる。
★「全打を記録する」のは、誰の役割か
ゴルフで本当に上達する人は、
ナイスショットに酔わない。
• フェアウェイキープ率
• パーオン率
• ミスの傾向
全打を見て、自分を知る。
医療と科学も同じだ。
• 効いた人
• 効かなかった人
• 副作用が出た人
これらすべてを含めて、
初めて「使っていい治療」になる。
だがSNSは、
全打を記録するのに向いていない。
★煽りが成立する理由は「責任がない」から
ナイスショットを語る人は、
次のラウンドの責任を取らない。
治療法を煽る投稿も同じだ。
• 効かなかった人は語らない
• 悪化した人は可視化されない
• 投稿は静かに流れて消える
だが、
身体は消えない。
ここに、
科学が絶対に手を抜けない理由がある。
★科学は「煽らない」ことを選んでいる
科学が地味なのは、
能力不足ではない。
• ナイスショットだけを語らない
• 恐怖だけで人を動かさない
• 希望を軽々しく売らない
この制約を、
自らに課している。
だから遅い。
だから静かだ。
だがそれは、
人の人生を賭け金にしない
という態度でもある。
★結論
治療法で煽るのも、
恐怖で煽るのも、
人間の脳の性質を
あまりにもよく知っているから成立する。
ナイスショットは、
記憶に残る。
だがスコアは、
積み上げで決まる。
健康も、人生も同じだ。
本当に信じるべきなのは、
一回の劇的な成功でも、
一瞬の恐怖でもない。
全体を見たときに、
再現性があり、
誰をも守れる選択かどうか。
ゴルフラウンドの帰り道、クラブケースを担ぎながら、ふとそんなことを思う。
科学とは、
ナイスショットを否定する学問ではない。
それに賭けていいかどうかを、
静かに問い直すためのスコアカードなのだ。
— Yet Why We Must Never Let Go of Evidence —
Scrolling through social media,
it often feels as though science is always losing.
“Dangerous!”
“This cures it!”
“The latest treatment doctors won’t tell you about!”
They are short, forceful, and emotionally charged.
By contrast, the language of science is slow, long, and cautious.
And so an illusion arises:
— perhaps science has become outdated.
But that is not the truth.
First and foremost,
science does not exist to win on social media.
What science values is:
Can it be reproduced?
Do others obtain the same results?
Could it be due to chance?
Does it still hold under different conditions?
In other words,
it prioritizes societal safety over individual excitement.
This stance inevitably dulls its language.
It cannot say, “This will definitely work.”
It cannot say, “There are no side effects.”
It cannot say, “Everyone will get the same result.”
This is not weakness.
It is evidence of taking responsibility.
The difference is only the sign.
One sells hope, the other sells anxiety.
Both press the same neural switches — the ones the human brain reacts to most strongly.
In golf:
Out of 100 shots, 99 are ordinary
Only one is truly perfect
Social media always cuts out that one shot.
“This treatment cured me.”
“This method changed my life.”
“You’re in danger if you don’t know this.”
The full picture,
the scorecard,
the reproducibility —
all of it disappears.
What remains is a single moment that feels good to believe.
Fear says:
“Don’t think — avoid.”
Hope says:
“Don’t think — believe.”
The directions differ,
but what happens in the brain is the same:
No comparison
No examination of conditions
No consideration of probabilities
That is why fear-based narratives and “new miracle treatments” spread at the same speed on social media.
Golfers who truly improve do not get drunk on perfect shots.
They look at:
Fairway hit rates
Greens in regulation
Patterns of mistakes
They examine every shot to understand themselves.
Medicine and science are the same.
Those for whom it worked
Those for whom it didn’t
Those who experienced side effects
Only when all of these are included
does a treatment become one that can be responsibly used.
Social media, however,
is not suited to recording every shot.
Those who boast about a perfect shot
take no responsibility for the next round.
Posts hyping treatments work the same way.
Those it didn’t help remain silent
Those who worsened are not made visible
The post quietly scrolls away and disappears
But the body does not disappear.
Here lies the reason science can never afford to cut corners.
Science is not dull because it lacks ability.
It does not speak only of perfect shots
It does not move people with fear alone
It does not sell hope lightly
These are self-imposed constraints.
That is why it is slow.
That is why it is quiet.
And that is also a stance:
not gambling with people’s lives.
Both treatment hype and fear-based messaging work
because they exploit the properties of the human brain with precision.
A perfect shot is memorable.
But a score is decided by accumulation.
Health, and life itself, are the same.
What we should truly trust
is not a single dramatic success,
nor a fleeting moment of fear.
It is whether, when viewed as a whole,
the choice is reproducible
and capable of protecting everyone.
Walking home after a round of golf,
carrying my club case,
this thought suddenly comes to mind.
Science is not a discipline that denies perfect shots.
It is a scorecard —
one that quietly asks
whether that shot is worth betting your life on.