検診大国・日本で、病気は減っているのか?
昨日、若手経営者とお酒をご一緒する機会があり、人間ドックや健康診断には行くべきかどうか、という話題になりました。
日本は世界でも突出した“検診大国”であり、これほど定期的に国民が健診を受けている国は、他にはほとんど存在しないと言ってよいでしょう。
まず結論から申し上げると、「死ななくはなったが、病気は減っていない」。
これが国際比較で見た、日本の実像であると感じます。
検診でわかるのは“早期発見”であって“予防”ではないということです。
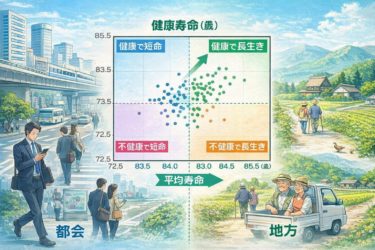
寿命と健康寿命の乖離
日本は平均寿命では長年、世界トップクラスを誇っています。
しかしながら、健康寿命との差、すなわち「不健康な期間」は決して短くありません。
日本の平均寿命:世界トップクラス
健康寿命との差:約9〜12年
この「長い不健康期間」は、病気を早く見つけ、その後も長く付き合っている結果ともいえます。
GBD Japan の解析でも、日本は
循環器疾患
糖尿病
筋骨格系疾患
といった慢性疾患の有病率が、高止まりしていることが明らかになっています。
検診は「発症を減らした」のか?
この問いに対しては、やや冷静に見る必要があります。
結論としては「重症化は減らしたが、発症そのものは減っていない」と言えるでしょう。
たとえば、がん検診では、早期がんの発見率は上昇し、5年生存率も改善しています。しかし一方で、年齢調整罹患率は横ばい〜微増という現象も確認されています。
これは過剰診断の影響も含め、病気の発症を減らすというよりも、「病気としてカウントされる期間を延ばしている」
という側面があると、New England Journal of Medicine(2012; 367:1995–2005)でも指摘されています。
日本の医療費は、どこに使われているのか?
次に浮かぶ疑問は、「保険診療だけでは医療機関がやっていけないから、検診や周辺医療で財務補填しているのではないか?」というものです。
この点については、半分正解と言えるかもしれません。
日本の保険診療は
診療単価が非常に低い
手間が診療報酬に反映されにくい
慢性疾患の長期管理では収益性が低い
といった構造的な制限を抱えています。
OECD の国際比較でも、日本は
医師の労働時間が長い
診療報酬単価が低い
という、いわゆる「高密度・低報酬モデル」とされています
(OECD Health at a Glance, 2023)。
その結果として、検診や画像診断、あるいは自費併用診療が、経営上の緩衝材になっている医療機関は少なくありません。
「病気を減らす」インセンティブの欠如
日本の医療システムをひと言で表すならば、「病気を減らすインセンティブが弱い構造」と言えるでしょう。
病気が早く見つかる → 医療行為が増える
長く通院する → 診療報酬が発生する
完全に健康 → 医療からの評価はゼロ
この構造では、予防が進めば進むほど、医療機関の収益は減ってしまいます。
Lancet の数字が示すこと
2019年、The Lancet に掲載されたGlobal Burden of Disease Study 2017 は、この問いに冷静かつ圧倒的なデータで答えを提示しました。
Global burden of 87 risk factors in 204 countries and territories, 1990–2017
The Lancet, 2019; 393:1958–1972
健康寿命を規定する因子の内訳は、おおよそ以下の通りです。
医療:10〜15%
遺伝:20%前後
生活・環境・社会構造:60%以上
つまり、「病院でどれだけ頑張っても限界がある」「健康は診察室の外で決まる」──
この結論は、もはや一部の極論ではありません。
予防医学や公衆衛生の世界では、共通認識として広く受け入れられているのです。
慢性疾患の多くは、症状が出る何年も前から、生活の中で静かに進行しているものです。
医療は非常に強力ですが、それは「壊れた後」に働く力であり、「壊さない力」ではありません。
──ここまでは、多くの専門家が一致する前提です。
意見A:だから、検診は意味がない
この前提に立つならば、
「検診をどれだけ受けても、健康にはなれない」
という結論に至るのは、むしろ自然な流れです。
検診で見つかるのは、すでに成立した病変、あるいはその直前の状態です。
しかし、その根本原因は生活の中にあり、検診では捉えきれません。
また、検診が高度化するほど、治療の必要がない異常や、経過観察で済む所見まで拾ってしまい、不安と医療介入がかえって増えてしまうことも知られています(New England Journal of Medicine, 2012; 367:1995–2005)。
健康は、数値を並べただけでは手に入りません。検診は「健康を作る手段」ではなく、単なる可視化に過ぎないのです。
もちろん、家族性のがんなど遺伝的リスクが高い方は、専門的な健診を受けるべきです。
反面、私が医師になった頃、国民的知名度を誇った日本テレビの逸見政孝アナウンサーは若くして胃がんで亡くなりました。
彼は家族歴から慎重で、半年に一度は胃カメラを飲んでいたそうです。それでも、病気は避けられなかったのです。
Lancet の数字を真正面から読むならば、「検診に力を注ぐ前に、生活構造そのものを変えるべきだ」という結論になるのです。
意見B:だからこそ、検診はした方がいい
とはいえ、同じ前提に立ちながら、違う結論に至ることもあるのです。
確かに、健康を決める最大の因子は「生活」です。
医療の寄与はたった10〜15%にすぎません。
しかし、その10〜15%こそが、「失敗が許されない領域」でもあるのです。
生活を整えていても
遺伝的素因
加齢
環境因子
といった要素によって、病気は一定の確率で起こります。
検診の役割は「健康を作ること」ではなく、「取り返しがつかなくなる前に逸脱を見つけること」です。
とくにがんや心血管疾患のように、発見時期で生存率や予後が大きく変わる病気に対しては、早期発見が生命を左右することが知られています(New England Journal of Medicine, 2013; 368:1279–1290)。
大切なのは、検診を「お守り」にしないことです。
検診を受けたから大丈夫、ではありません
生活が整っているから検診は不要、でもありません
Lancet の数字は、検診そのものを否定しているのではなく、検診の位置づけを正しく捉えなさいと警鐘を鳴らしているのです。
あなたは、どちらを信じますか?
意見Aと意見B。
正反対のようで、どちらも医学的に根拠があります。
どちらの道を選ぶかは、あなたが健康をどう捉えるかにかかっています。
未来の自分の健康を、検査室に任せるか、あるいは日々の生活の中で作り上げていくか──その選択の一助になれば幸いです。

Does Disease Really Decrease in “Health Checkup Nation” Japan?
Yesterday, I had the opportunity to share drinks with a group of young business leaders, and the topic came up as to whether one should undergo regular medical checkups and comprehensive health screenings. Japan is an exceptionally prominent “health checkup nation,” and it would not be an exaggeration to say that few other countries have populations that undergo routine medical examinations as regularly as Japan does.
To begin with the conclusion: people have become less likely to die, but disease itself has not decreased. This, in my view, is the true picture of Japan when seen through international comparison. What health checkups provide is early detection, not prevention.
The Gap Between Life Expectancy and Healthy Life Expectancy
Japan has long boasted one of the highest average life expectancies in the world.
However, the gap between life expectancy and healthy life expectancy—that is, the period of life spent in poor health—is by no means short.
Average life expectancy in Japan: among the highest globally
Gap with healthy life expectancy: approximately 9–12 years
This long period of ill health can also be understood as the result of detecting diseases early and then living with them for a long time thereafter.
Analyses by GBD Japan have shown that the prevalence of chronic diseases such as
cardiovascular disease,
diabetes, and
musculoskeletal disorders
remains persistently high in Japan.
Have Health Checkups Reduced the Onset of Disease?
This question requires a calm and measured assessment.
The conclusion is that health checkups have reduced disease severity, but not disease incidence itself.
For example, in cancer screening, detection rates of early-stage cancers have increased and five-year survival rates have improved. At the same time, however, age-adjusted incidence rates remain flat or have slightly increased.
This phenomenon—including the effects of overdiagnosis—suggests that rather than reducing disease occurrence, screening may be extending the period during which a condition is labeled as a disease. This point was also noted in the New England Journal of Medicine (2012; 367:1995–2005).
Where Is Japan’s Medical Spending Going?
A natural follow-up question is whether medical institutions rely on health checkups and ancillary services to compensate financially because insurance-based medical care alone is unsustainable. On this point, the answer may be partly yes.
Japan’s insurance-based medical system faces structural constraints, including:
extremely low unit prices for medical services,
insufficient reflection of labor intensity in reimbursement, and
low profitability in the long-term management of chronic diseases.
International comparisons by the OECD characterize Japan as a so-called “high-density, low-compensation model,” marked by long physician working hours and low reimbursement rates (OECD Health at a Glance, 2023).
As a result, many medical institutions use health checkups, diagnostic imaging, and mixed private-pay services as financial buffers.
The Lack of Incentives to “Reduce Disease”
If Japan’s healthcare system were to be summarized in one phrase, it would be a structure with weak incentives to reduce disease.
Early detection of disease → more medical interventions
Long-term outpatient care → continued reimbursement
Perfect health → no evaluation from the medical system
In this structure, the more prevention succeeds, the more medical revenue declines.
What the Lancet Data Show
In 2019, The Lancet published the Global Burden of Disease Study 2017, which addressed this issue with overwhelming data:
Global burden of 87 risk factors in 204 countries and territories, 1990–2017
(The Lancet, 2019; 393:1958–1972)
The approximate breakdown of factors determining healthy life expectancy is as follows:
Medical care: 10–15%
Genetics: around 20%
Lifestyle, environment, and social structure: over 60%
In other words, there is a clear limit to what hospitals can do, and health is largely determined outside the examination room. This conclusion is no longer an extreme view, but a widely accepted consensus in preventive medicine and public health.
Most chronic diseases progress quietly within daily life for years before symptoms appear. Medicine is extraordinarily powerful, but it is a force that works after something has broken, not a force that prevents it from breaking. Up to this point, most experts are in agreement.
Opinion A: Therefore, Health Checkups Are Meaningless
From this premise, it is almost natural to conclude that no matter how many checkups one undergoes, they do not lead to health.
What checkups detect are already established lesions or states immediately preceding them. Their root causes lie in daily life and cannot be fully captured by screening. Moreover, as screening becomes more sophisticated, it also detects abnormalities that require no treatment or only observation, increasing anxiety and unnecessary medical intervention (NEJM, 2012; 367:1995–2005).
Health cannot be obtained simply by lining up numerical values. Health checkups are not a means of creating health; they are merely a form of visualization.
Of course, individuals with high genetic risk—such as familial cancer—should undergo specialized screening. On the other hand, Masataka Itsumi, a widely known Japanese television announcer when I first became a physician, died young of gastric cancer. He was cautious due to family history and reportedly underwent gastroscopy every six months. Even so, the disease could not be avoided.
If one reads the Lancet data head-on, the conclusion is clear: before investing more in checkups, we should change the structure of daily life itself.
Opinion B: Precisely Because of That, You Should Get Checkups
That said, starting from the same premise can also lead to a different conclusion.
It is true that lifestyle is the dominant determinant of health, and medical care contributes only 10–15%. However, that 10–15% represents a domain where failure is not acceptable.
Even with a well-regulated lifestyle, disease occurs at a certain probability due to:
genetic predisposition,
aging, and
environmental factors.
The role of health checkups is not to create health, but to detect deviations before they become irreversible. For diseases such as cancer and cardiovascular conditions—where timing of detection dramatically affects survival and prognosis—early detection can be decisive (NEJM, 2013; 368:1279–1290).
What matters is not turning checkups into a talisman.
Having a checkup does not mean you are safe.
Having a good lifestyle does not mean checkups are unnecessary.
The Lancet data do not deny health checkups themselves; they warn us to position them correctly.
So, which do you believe?
Opinion A or Opinion B.
They appear to be opposites, yet both are medically grounded.
Which path you choose depends on how you define health.
Will you entrust your future health to the examination room,
or will you build it day by day through your daily life?
I hope this helps inform that choice.