





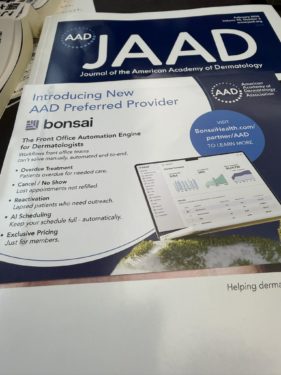
毎月学会員に送られてくるAAD 米国皮膚科学会の機関誌。
表紙を見て、まず目に飛び込んできたのは「Introducing New AAD Preferred Provider」という一文でした。
その下には「bonsai」という、どこか日本的な名前のサービスが紹介されています。
一瞬、違和感がよぎります。
なぜ、盆栽なのだろうか。
■ 盆栽という思想の再輸入
日本人にとって盆栽とは、単なる趣味ではありません。
自然をそのままにするのではなく、意図的に手を加え、時間をかけて最適な形へと導いていく行為です。
・不要な枝を落とす
・弱った部分を再生させる
・全体のバランスを整える
これは驚くほど、その広告に書かれている内容と一致しています。
予約の空白を減らす
無断キャンセルを抑制する
離脱患者を呼び戻す
スケジュールを最適化する
つまりこれは、患者という「流れ」を整える技術であり、言い換えれば医療経営の盆栽化だといえます。
■ 「Preferred」という絶妙な距離感
ここでさらに興味深いのが、「Preferred」という言葉です。
直訳すれば「好ましい」「優先される」ですが、
アメリカの文脈ではもう少し複雑な意味を持ちます。
Certified(認定)ではない
Approved(承認)でもない
しかし無関係でもない
つまりこれは、信頼を感じさせながら、責任は限定する言葉です。
実際、米国の学会誌に掲載されるこうしたサービスの多くは、臨床的な有効性を保証されているわけではありません。一定の審査や関係性の中で紹介されているに過ぎません。
それでもなお、「Preferred」という一語が付くことで、読者である医師の心理には微妙な安心感が生まれます。
この“余白の設計”こそ、実にアメリカ的だと感じます。
■ 医療は技術か、システムか
もう一つ重要なのは、医療の捉え方の違いです。
日本では、医療はしばしば、「医師の技術」として語られます。
一方、アメリカでは明確に異なります。医療はシステムであると捉えられています。
とりわけ外来診療においては、
No-show(無断キャンセル)
患者回転率
再来率
といった要素が、そのまま経営に直結します。
実際、皮膚科外来におけるNo-show率は10〜30%に達するとの報告もあり、これを改善することは単なる効率化ではなく、収益構造そのものの改善を意味します。
ここにおいて、「bonsai」は単なるITツールではありません。
それは、医療の流れを設計する装置なのです。
■ 見えない部分を整えるという発想
盆栽の本質は、“見えない部分”にあります。根の状態、水分、土壌環境。外からは見えないが、すべてを決定する要素です。
これは医療経営においても同じです。
患者の行動履歴
来院パターン
離脱リスク
予約の空白
こうしたデータを解析し、最適化していく。
それはまさに、データによる盆栽管理といえるでしょう。
興味深いことですね。
The Structure of American Medicine Embedded in a Single Word: “Preferred”
Every month, members receive the official journal of the American Academy of Dermatology (AAD).
As I glanced at the cover, one phrase immediately caught my eye:
“Introducing New AAD Preferred Provider.”
Beneath it was a service with a somewhat Japanese-sounding name: “bonsai.”
For a moment, I felt a slight sense of dissonance.
Why bonsai?
■ The Re-importation of the Bonsai Philosophy
For Japanese people, bonsai is not merely a hobby.
It is the act of not leaving nature untouched, but instead deliberately shaping it over time into its optimal form.
Pruning unnecessary branches
Revitalizing weakened parts
Adjusting the overall balance
Surprisingly, this aligns almost perfectly with what the advertisement describes:
Reducing gaps in appointment schedules
Preventing no-shows
Re-engaging patients who have dropped out
Optimizing scheduling
In other words, this is a technology for shaping the “flow” of patients—
or, put differently, the bonsai-ization of healthcare management.
■ The Subtle Distance Implied by “Preferred”
What makes this even more interesting is the word “Preferred.”
A direct translation might be “favorable” or “prioritized,”
but in the American context, it carries a more nuanced meaning:
Not “Certified”
Not “Approved”
Yet not unrelated
It is a term that conveys trust while limiting responsibility.
In reality, many such services featured in U.S. academic journals are not guaranteed for clinical efficacy. They are simply introduced within a certain framework of review or affiliation.
And yet, the addition of the single word “Preferred” creates a subtle sense of reassurance in the minds of physician readers.
This “design of ambiguity” feels distinctly American.
■ Is Medicine a Skill, or a System?
Another important point lies in how medicine itself is perceived.
In Japan, medicine is often discussed as the “skill of the physician.”
In contrast, in the United States, medicine is clearly regarded as a system.
Particularly in outpatient care, factors such as:
No-shows
Patient turnover rate
Return visit rate
are directly tied to management outcomes.
In fact, reports suggest that no-show rates in dermatology clinics can reach 10–30%. Improving this is not merely a matter of efficiency—it directly transforms the revenue structure itself.
In this context, “bonsai” is not just an IT tool.
It is a mechanism for designing the flow of healthcare.
■ The Philosophy of Managing the Invisible
The essence of bonsai lies in what cannot be seen:
the condition of the roots, moisture levels, the soil environment.
These invisible elements ultimately determine everything.
The same holds true in healthcare management:
Patient behavior histories
Visit patterns
Risk of dropout
Gaps in scheduling
Analyzing and optimizing these elements—
this is, in essence, bonsai management through data.
Fascinating, isn’t it?