





「いちごは春の小さな処方箋」
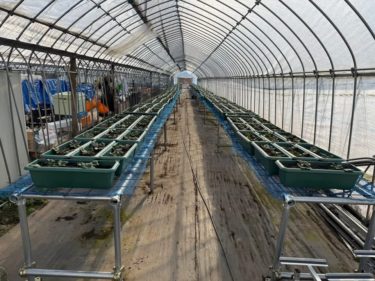
晴天の今日は、ご縁をいただいた「いちご農家」の見学に農学部で学ぶ次男と行ってきました。イメージしていたよりはるかに巨大な施設。なかなか観られない経験に感激。思えば、日本ほど美味しいいちごは、海外では滅多に食べられません。




お土産にいただいたいちごをみて、「これは栄養学的にどれだけ価値があるのだろう」と、つい研究者の癖が顔を出しました。
そんなわけで、いちごの栄養価を、整理してみました。
●いちごの主要な栄養価
成分 期待できる作用
ビタミンC(約62mg/100g) 抗酸化・免疫支持・コラーゲン合成の素材に
アントシアニン 血管・脳・視機能のサポート
エラグ酸 肌の光老化抑制に関連
食物繊維 腸内環境の補助、食後血糖の急上昇抑制に一役
カリウム ナトリウム調整による血圧サポート
●医学的メリット
▲抗酸化と細胞保護
ローマの研究グループは、いちご摂取で血中抗酸化能が上昇し、炎症・酸化ストレス指標が改善する可能性を示した。
→ Giampieri F et al., Journal of Agricultural and Food Chemistry, 2012, 60:6120–6130.
▲心血管リスクの低減に関与する可能性
フラボノイド(いちご・ブルーベリー由来)の摂取が、若年~中年女性における心筋梗塞リスク低下と関連。
→ Cassidy A et al., American Journal of Clinical Nutrition, 2013, 97(1):176–185.
▲整肌作用(光老化の抑制)
紫外線によるコラーゲン分解を、いちご由来エラグ酸が阻害する可能性を示した基礎研究。
→ Bae J et al., Journal of Investigative Dermatology, 2010, 130(6):1465–1472.
▲糖制御の補助(GIが低め)
食後血糖の上昇抑制を示唆する報告。糖質はあるが、食物繊維と低GIが救いになる。
→ Edirisinghe I et al., Journal of Medicinal Food, 2011, 14(5):510–517.
▲農法による抗酸化能の違い
有機栽培いちごの方が抗酸化成分が高い可能性。選び方のヒントに。
→ Asami DK et al., Journal of Agricultural and Food Chemistry, 2003, 51(5):1237–1241.
良い事ばかりじゃないか!
いちごは甘すぎるんじゃないかと思い、気になる実際の糖量はを調べてみましたが、いちご100gあたりの糖質は約7.5g前後。果物の中では比較的低めの部類。
食材 糖質量(約)
いちご 100g 7.4–7.5g
バナナ 100g 21.4g
みかん 100g 10.9g
ぶどう 100g 15.2g
引用
→ USDA National Nutrient Database, Release 28 (2016)
つまり、「甘いけど重くない」は数字にも裏付けがある。
●なぜ甘く感じるのか
・クエン酸の酸味が、味覚神経の閾値を下げて甘味を強調
・ビタミンCの清涼感が後味を引き締める
・品種改良で“香りのボリューム”が増し、香りが甘味を補強する
香りと酸味の構造が、脳内で甘さの印象を増幅している。
これを示唆する実験もある。
→ Schifferstein HN et al., Chemical Senses, 2002, 27(7):613–624.
●血糖値の観点では?
いちごのGI値は約40(低GI)。
→ Atkinson FS et al., American Journal of Clinical Nutrition, 2008, 87(1):247S–253S.
もちろん量や食べ方によるが、同カロリーの砂糖菓子より血糖負荷は穏やかである。
「甘いけれど、身体に優しい範囲で完結する甘さ」
糖としての負担は控えめだが、感覚としての満足度は高い。
このギャップこそが、いちごの上品さであり、春の果物らしい“節度の美学”と言えますね。
日本の農家でも、いちごには未来はありますね!
“Strawberries: A Small Springtime Prescription”
On this beautifully clear day, I visited a strawberry farm I had the good fortune to be connected with, together with my second son, who studies agriculture at university.
The facility was far larger than I had imagined—an impressive experience that one rarely gets to see.
Come to think of it, strawberries as delicious as those in Japan are rarely found overseas.
Looking at the strawberries we received as a gift, the researcher in me instinctively surfaced:
“Just how valuable are these nutritionally?”
So, I decided to organize the nutritional profile of strawberries.
Key Nutritional Components of Strawberries
| Component | Expected Effects |
|---|---|
| Vitamin C (~62 mg/100 g) | Antioxidant activity, immune support, and a substrate for collagen synthesis |
| Anthocyanins | Support for blood vessels, brain health, and visual function |
| Ellagic acid | Associated with suppression of photoaging of the skin |
| Dietary fiber | Supports gut health and helps moderate postprandial blood glucose spikes |
| Potassium | Supports blood pressure regulation via sodium balance |
Medical and Scientific Benefits
▲ Antioxidant and Cellular Protection
A research group in Rome demonstrated that strawberry consumption may increase plasma antioxidant capacity and improve markers of inflammation and oxidative stress.
→ Giampieri F et al., Journal of Agricultural and Food Chemistry, 2012, 60:6120–6130.
▲ Potential Reduction in Cardiovascular Risk
Intake of flavonoids (from strawberries and blueberries) was associated with a reduced risk of myocardial infarction in young to middle-aged women.
→ Cassidy A et al., American Journal of Clinical Nutrition, 2013, 97(1):176–185.
▲ Skin-Conditioning Effects (Suppression of Photoaging)
Basic research suggests that ellagic acid derived from strawberries may inhibit UV-induced collagen degradation.
→ Bae J et al., Journal of Investigative Dermatology, 2010, 130(6):1465–1472.
▲ Support for Glycemic Control (Relatively Low GI)
Reports suggest strawberries may help suppress postprandial blood glucose rises. While they do contain carbohydrates, dietary fiber and a low GI offer protection.
→ Edirisinghe I et al., Journal of Medicinal Food, 2011, 14(5):510–517.
▲ Differences in Antioxidant Capacity by Farming Method
Organically grown strawberries may contain higher levels of antioxidant compounds—useful information when choosing produce.
→ Asami DK et al., Journal of Agricultural and Food Chemistry, 2003, 51(5):1237–1241.
So many benefits—almost too good to be true!
But Aren’t Strawberries Too Sweet?
Curious about the actual sugar content, I looked it up. Strawberries contain approximately 7.5 g of carbohydrates per 100 g, which is relatively low among fruits.
| Food | Carbohydrates (approx.) |
|---|---|
| Strawberries (100 g) | 7.4–7.5 g |
| Bananas (100 g) | 21.4 g |
| Mandarins (100 g) | 10.9 g |
| Grapes (100 g) | 15.2 g |
Source:
→ USDA National Nutrient Database, Release 28 (2016)
In other words, “sweet, yet not heavy”—a claim supported by numbers.
Why Do Strawberries Taste So Sweet?
-
Citric acid lowers the sensory threshold of taste receptors, enhancing perceived sweetness
-
Vitamin C provides a refreshing finish that sharpens the aftertaste
-
Breeding has increased the “volume” of aroma, with fragrance reinforcing sweetness
The interplay of aroma and acidity amplifies the perception of sweetness in the brain.
Experiments supporting this mechanism have been reported.
→ Schifferstein HN et al., Chemical Senses, 2002, 27(7):613–624.
From a Blood Glucose Perspective
Strawberries have a GI value of approximately 40, classifying them as a low-GI food.
→ Atkinson FS et al., American Journal of Clinical Nutrition, 2008, 87(1):247S–253S.
Of course, quantity and timing matter, but compared with sugary confections of equal calories, strawberries impose a gentler glycemic load.
In Summary
“Sweet, yet gentle on the body.”
The metabolic burden of sugar is modest, while sensory satisfaction remains high.
This gap is precisely what gives strawberries their elegance—a kind of aesthetic of moderation that feels quintessentially springlike.
Even for Japanese farmers, the future of strawberries looks bright.